About Hunterase
What is
Hunterase?
Composition
Active ingredient : Idursulfase-β 6.0 mg (3 ml in 1 vial)Indication
Hunterase (Idursulfase-β) is indicated for patients with Hunter Syndrome (Mucopolysaccharidosis II, MPS II) as an enzyme replacement therapy (ERT).Clinical Trials
Hunterase (Idursulfase beta) is a safe and effective treatment option in mucopolysaccharidosis II (MPS II),
addressing crucial somatic ailments presented by patients.
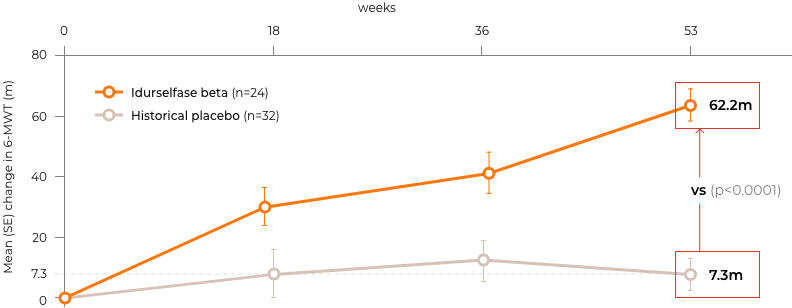
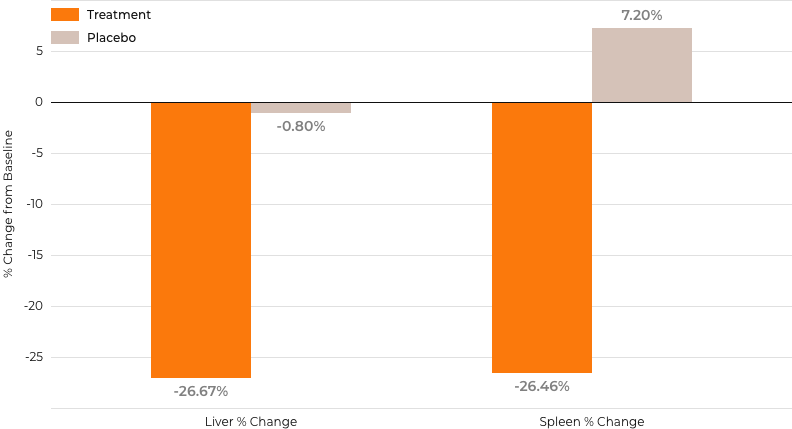
In Phase III, participants in the idursulfase beta groups (n = 24) were male Asians (mean age, 12.0 years). Idursulfase beta was superior to placebo in 6-minute walk test improvement (62.2 vs 7.3 m, P < .0001). Decrease in urine glycosaminoglycan excretion (-71.13% vs 21.39%, P < .0001) and reduction in the liver (-26.67% vs -0.80%, P < .0001) and spleen volumes (-26.46% vs 7.2%, P < .0001) were significant.
The safety profile of idursulfase beta was satisfactory.
This study demonstrated the superiority of idursulfase beta over placebo in improving 6-MWT results. Furthermore, idursulfase beta significantly reduced urine GAG excretion and liver and spleen volumes while exhibiting a safety profile comparable to that of idursulfase.
In Phase III, participants in the idursulfase beta groups (n = 24) were male Asians (mean age, 12.0 years). Idursulfase beta was superior to placebo in 6-minute walk test improvement (62.2 vs 7.3 m, P < .0001). Decrease in urine glycosaminoglycan excretion (-71.13% vs 21.39%, P < .0001) and reduction in the liver (-26.67% vs -0.80%, P < .0001) and spleen volumes (-26.46% vs 7.2%, P < .0001) were significant.
The safety profile of idursulfase beta was satisfactory.
This study demonstrated the superiority of idursulfase beta over placebo in improving 6-MWT results. Furthermore, idursulfase beta significantly reduced urine GAG excretion and liver and spleen volumes while exhibiting a safety profile comparable to that of idursulfase.




*Historical placebo cohort from a previous idursulfase trial (TKT024)2
R,
randomization; Tx, treatment; f/u, follow-up; MPS II, mucopolysaccharidosis type II.
randomization; Tx, treatment; f/u, follow-up; MPS II, mucopolysaccharidosis type II.
Methods
The study comprised two sequential parts.In Part 1,
a randomized, double-blind study,idursulfase or idursulfase beta were given for 52 weeks.
In the open, single cohort Part 2 study,
additional participants received idursulfase beta for 52 weeks.Data from the idursulfase beta groups from Parts 1 & 2 were pooled for comparisons with the historical placebo group (n=32)
Primary endpoint
A change in the 6-minute walk test(6-MWT) at week 53
Secondary endpoints
Changes in:- 6MWT at other time points
- Urine total GAG levels
- Heparan sulfate (HS) and Dermatan sulfate (DS) levels
- Liver volume
- Spleen volume
- Absolute forced vital capacity (FVC)
- Echocardiographic parameters assessing cardiac size and function
Primary Endpoint and Results
The mean change at week 53 in the idursulfase beta group demonstrated the superiority compared to the
histrorical placebo group.
Idursulfase group was significantly greater than that in the historical placebo group (62.2 vs 7.3 m, P < .0001), with a lower bound of the 1-sided 95% CI of 48.05 m.
Per-protocol analysis showed a similar level of significant change in the idursulfase beta group (mean = 62.1 m, median = 52.8 m).
Idursulfase group was significantly greater than that in the historical placebo group (62.2 vs 7.3 m, P < .0001), with a lower bound of the 1-sided 95% CI of 48.05 m.
Per-protocol analysis showed a similar level of significant change in the idursulfase beta group (mean = 62.1 m, median = 52.8 m).
Changes in 6-minute walk test (6MWT) throughout the study period
*Historical placebo from a previous idursulfase trial (TKT024)²
Secondary Endpoints and Results
Mean percent change in urine total GAG concentration at week 53 showed a
significant reduction in the idursulfase beta group compared with that in the historical placebo
group (-71.13% vs 21.39%, P < .0001)
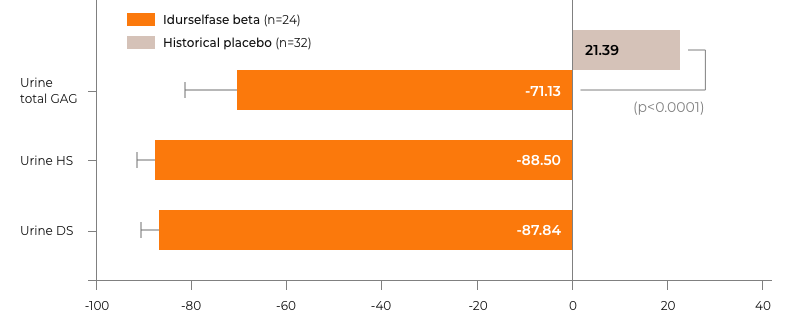
% changes in urine total GAG, HS, and DS level at week 53
The error bar represents a 90% CI.
*Historical placebo from a previous idursulfase trial (TKT024)²
GAG, glycosaminoglycan
*Historical placebo from a previous idursulfase trial (TKT024)²
GAG, glycosaminoglycan
% changes in Liver and Spleen Volume at week 53
Immunogenicity
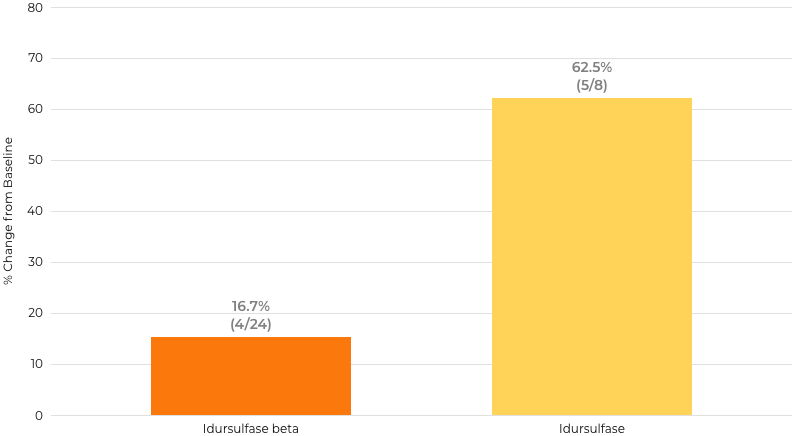
Idursulfase beta showed a lower rate of persistent NAb+ (16.7% vs
62.5%) compared with idursulfase, and in the beta group, NAb− patients had slightly
greater HS/DS reductions, while NAb+ patients experienced more SAEs and acute
AEs.
 Proportion of patients with neutralizing antibody positivity (NAb+) in the
idursulfase beta group (A) or idursulfase group (B). a Only when an antidrug antibody (ADA) test was
positive, an NAb test was carried out subsequently.
Proportion of patients with neutralizing antibody positivity (NAb+) in the
idursulfase beta group (A) or idursulfase group (B). a Only when an antidrug antibody (ADA) test was
positive, an NAb test was carried out subsequently.
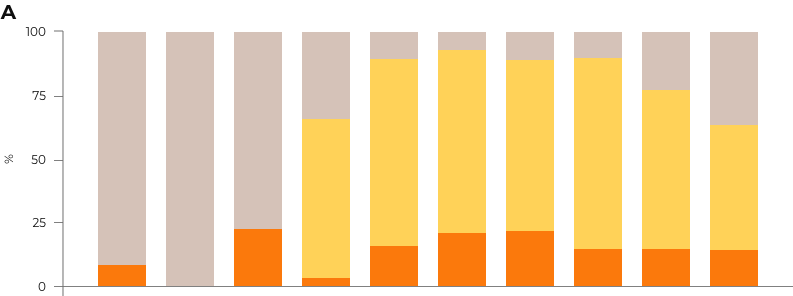
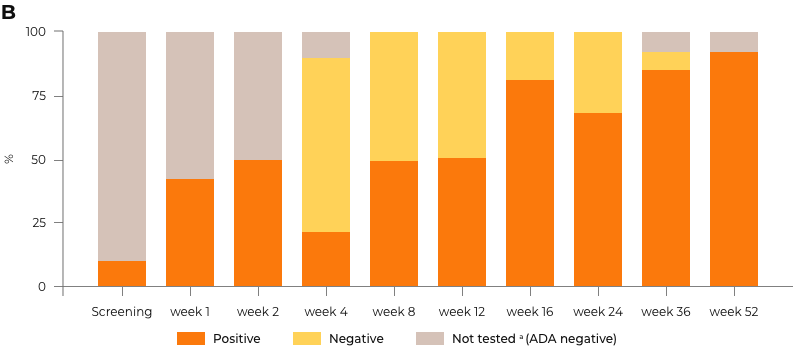
Persistent NAb+ Proportion by Treatment Group
Idursulfase beta (n=24)
Idursulfase (n=8)
Safety
In the idursulfase beta group, most adverse events were mild to moderate with no
treatment discontinuations, and the proportion of patients with persistent neutralizing antibodies
during the treatment period was 16.7%, notably lower than 62.5%
observed with the active comparator.
|
Idursulfase beta (Parts 1&2) (n=24) |
Idursulfase (Part 1) (n=8) |
|
|---|---|---|
| Anti-drug antibodies, n(%) | ||
| Positive at least once | 23 (95.8) | 8 (100.0) |
| Positive ≥ three times consecutively | 21 (87.5) | 8 (100.0) |
| Neutralizing antibodies [Neutralizing assay], n(%) | ||
| Positive at least once | 9 (37.5) | 8 (100.0) |
| Positive ≥ three times consecutively | 4 (16.7) | 5 (62.5) |
Safety Information
Hunterase should be administered by a healthcare professional
according to the prescribing information.
PRECAUTIONS
Storage And
Shelf-life
- Store at a 2 ºC to a 8 ºC in a hermetic container.
- The shelf-life of this product is 36 months from the date of manufacture.
ADVERSE
REACTIONS
- All adverse reactions in patients treated with Hunterase weekly for 24 weeks compared with the active comparator during the clinical trial are shown in the pdf file below. 3 serious adverse reactions were observed: 2 cases of otitis media and 1 case of gastroenteritis. However, all cases were determined as ‘not-related’ to Hunterase.
- Adverse reactions associated with Hunterase were urticaria, rashes, and pruritus.
All adverse reactions were mild and controlled by adjusting the infusion rate and using proper drug treatments.
ENG Official Insert Paper


How to Use
Recommended Dosage
- Method: intravenous infusion, once weekly.
- Each vial of Hunterase contains 2 mg/ml of Idursulfase-β.
One vial contains 6 mg of Idursulfase-β in 3 ml solution and is for single use only. - Recommended dosage of Idursulfase-β protein = Patient’s weight (kg) * 0.5 mg/kg
Automatic Calculation
Enter your weight and it will be calculated automatically.
1 ml

Hunterase 1 Vial
Idursulfase-ß 6.0 mg / 3 mL
Idursulfase-ß 6.0 mg / 3 mL
Please enter your weight (kg)
kg

Recommended dosage of Idursulfase-β = Patient’s weight (kg) * 0.5 mg/kg
Idursulfase-β (mg)
mg
Hunterase (vial)
vials
Injection Process
This information is based on the common clinical practice. It is not published or written in the package insert.
01
Open the Hunterase Vial(s) after determining the required number of vials using
the above calculator.
02
Sterile the Hunterase Vial Cap.
03
Dilute Hunterase in 100 ml of normal saline (0.9% sodium chloride injection) in
the infusion bag.
04
Adjust the infusion rate considering the patient’s condition.
Recommendation
The initial infusion rate for the first 15 minutes – 8 mL/hr. If the infusion is well tolerated, the rate may be increased by 8 mL/hr increments every 15 minutes. The infusion rate should not exceed 100 mL/hr.Precautions in Storage and Handling
- Store Hunterase vials under refrigeration at 2 ºC to 8 ºC
- Protect from light without freezing and do not shake it.
- Do not use Hunterase after the expiration date on the vial.
- This product contains no preservatives. The diluted solution should be used immediately. If immediate use is not possible, the diluted solution can be stored refrigerated at 2 ºC to 8 ºC for up to 48 hours, or must be administered within 8 hours if held at room temperature.
References
- Orphanet J Rare Dis. 2013;8:42
- Mol Ther Methods Clin Dev. 2021;21:67-75
- Mol Genet Metab. 2015;114(2):156-60
Contact us
For More Information,
Please
Contact Us.
Please
Contact Us.

Address
107 Ihyeon-ro 30-beongil, Giheung-gu, Yongin-si,
Gyeonggi-do Republic of Korea
Contact

© Hunterase ALL RIGHTS RESERVED


